Volunteered for Something
30/04/25 08:14
Well I hadn’t heard from anyone about the proposal to change of medication from the Copaxone syringes to the Tecfidera tablets, but it was always going to take quiet a while for discussions and approvals getting in place. But on Friday I got a call asking if I’d be interested in joining a survey program for a study being undertaken at the Walton Centre, which would involve me getting various additional blood tests and I think potentially more MRI/CT scans. I’m not sure yet what I’ve agreed to, but if me getting tested helps any understanding of the damn disease and its treatment then it’s got to be a good thing, ain’t it?
At the end of the phone call I asked if the approval was going through yet. Of course it turned out that’s why they’ve asked me to join the study (which they kept saying was voluntary and I didn’t need to do), it’s because the medication change has indeed been confirmed. Not sure yet when it’ll start but before too long anyway. Fingers crossed the mediation arrives soon and will be a help and not have too many side effects (or at least not bad ones).
Onwards and Upwards.
At the end of the phone call I asked if the approval was going through yet. Of course it turned out that’s why they’ve asked me to join the study (which they kept saying was voluntary and I didn’t need to do), it’s because the medication change has indeed been confirmed. Not sure yet when it’ll start but before too long anyway. Fingers crossed the mediation arrives soon and will be a help and not have too many side effects (or at least not bad ones).
Onwards and Upwards.
Comments
Meditation on Medication
14/03/25 16:30
After well over a year between Walton Centre visits I’ve just had two visits within four weeks. During the last one there was some talk about taking a drug (Aubagio) to replace the Copaxone I’ve been on—in light of a recent relapse. When I took a phone call the other week the talk was about a different drug; Tecfidera (dimethyl fumarate). I assume that the addition of a different possibility was after the nurse had spoken to the consultant. The centre sent me a detailed guide to the drug to help my considerations.
There are a quite a few things to consider with the medication (Tecfidera). There are plenty of possible side effects some more common, some quite serious. And the way that the drug works and can impact on people means that there will need to be quarterly blood tests in order to identify potentially significant issues. The more common ones (c.1 in 10) are gastric ones, flushing, and hair loss is listed too. The more significant ones include PML (the mighty mouthful of ‘progressive multifocal leukoencephalopathy), which is where the blood tests come in. It’s handy living near to the Walton Centre as I should just be able to pop in there every 3 months and get the samples taken without messing about with booking appointments (often a more painful experience than the actual needle in the arm).
Interestingly they know that the drug works but they don’t understand completely why. Like Viagra the drug was actually designed for something else (psoriasis) and subsequently found to be useful in the treatment of MS.
Anyways all the side effects are possibilities not guaranteed effects, in any case maybe I’d look good red faced and bald. The main thing is the drug will likely do a better job than Copaxone and—importantly—actually treat the MS to some extent, and not just reduce the risk of a relapse, so I’ve decided to go for it. It’s a no brainer really.
First up was some blood sampling—taken today whilst there—to see if my body is up to it and also to set a baseline. There may be an MRI (but probably not).
It’ll probably be a month or so until I get on it. First the bloods results, then various toing and froing between people for approving and issuing the prescription then getting it ordered (the same home delivery company a those that deliver the Copaxone). The first few months on the drug may be interesting, but even if there are some negative impacts hopefully things would settle down after that. Fingers crossed for everything.
There are a quite a few things to consider with the medication (Tecfidera). There are plenty of possible side effects some more common, some quite serious. And the way that the drug works and can impact on people means that there will need to be quarterly blood tests in order to identify potentially significant issues. The more common ones (c.1 in 10) are gastric ones, flushing, and hair loss is listed too. The more significant ones include PML (the mighty mouthful of ‘progressive multifocal leukoencephalopathy), which is where the blood tests come in. It’s handy living near to the Walton Centre as I should just be able to pop in there every 3 months and get the samples taken without messing about with booking appointments (often a more painful experience than the actual needle in the arm).
Interestingly they know that the drug works but they don’t understand completely why. Like Viagra the drug was actually designed for something else (psoriasis) and subsequently found to be useful in the treatment of MS.
Anyways all the side effects are possibilities not guaranteed effects, in any case maybe I’d look good red faced and bald. The main thing is the drug will likely do a better job than Copaxone and—importantly—actually treat the MS to some extent, and not just reduce the risk of a relapse, so I’ve decided to go for it. It’s a no brainer really.
First up was some blood sampling—taken today whilst there—to see if my body is up to it and also to set a baseline. There may be an MRI (but probably not).
It’ll probably be a month or so until I get on it. First the bloods results, then various toing and froing between people for approving and issuing the prescription then getting it ordered (the same home delivery company a those that deliver the Copaxone). The first few months on the drug may be interesting, but even if there are some negative impacts hopefully things would settle down after that. Fingers crossed for everything.
MS Stress
23/02/25 14:06
Went to the wonderful Walton Centre for a meeting with a couple of the MS Nurses a week or so ago. All in all it was an interesting appointment.
My MS has been steady for the last few years, but over the last few weeks I have been suffering from my first relapse since my initial two relapses, which was back when I was diagnosed.
For those of you who don’t know, a ‘relapse’ is not (as it sounds) a return to any earlier symptoms but relates to something different—a symptom that you haven’t had before. The current relapse is an almost total numbness of the lower torso from above the belly button height and all around from back to front. It is also partially down my left leg. The attack of course is to my nerves (the myelin coating) on the spine or in the brain (or both) in specific areas. In this case it appears to be nerves near the base of the spine.
It’s weird not feeling the syringe with the Copaxone going in to the belly. Whilst not feeling the injection sounds quite nice, it’s not exactly, is it? Not feeling your torso is disorientating at the moment and has other issues relating to it. I am hopeful, as in the previous attacks, that most of the feeling will come back over the next few weeks; but the return of the RRMS has left me pretty stressed to be honest.
One thing that came up in discussion was the issue I have with fatigue when standing up for over an hour or so (eg at a gig). It created much hilarity when the nurse suggested that one of the best ways to reduce the fatigue was to piss myself. I was quite taken aback by this suggestion until after some requests for repetition I found it was an accent issue and she’d actually meant ‘pace’. Much better idea I reckon.
They’ve written a letter for me which I hope to use to apply for an Access Card to help my when attending events (with better access to toilets and seats etc). I’d had to put off going to the Lottery Winners gig at Manchester Academy between Xmas and New Year because I was too worried that I wouldn’t find a place to sit (I was using a walking stick at the time). I was gutted at missing it but it was the correct decision at the time. We shall see whether I, a) get one and b) if it’s worth getting.
Another discussion was around possibly changing my medication from the three times a week Copaxone (glatiramer acetate) injections to daily tablets (Aubagio—terifluomide). When I first went for the injections it was partly due to the worry about purposely lowering your white blood cell count and also requiring regularly blood testing (not required with the Copaxone treatment). Given I am currently attacking myself again lowering the White Blood Cells doesn’t seem as bad an idea at all. The nurse is to call me back over the next few weeks and I am currently minded to opt for the change to Aubagio after the next batch of Copaxone is completed. We shall see.
Watch this space. In the meantime though I need to take some deep, deep breaths and try to stress less in general.
My MS has been steady for the last few years, but over the last few weeks I have been suffering from my first relapse since my initial two relapses, which was back when I was diagnosed.
For those of you who don’t know, a ‘relapse’ is not (as it sounds) a return to any earlier symptoms but relates to something different—a symptom that you haven’t had before. The current relapse is an almost total numbness of the lower torso from above the belly button height and all around from back to front. It is also partially down my left leg. The attack of course is to my nerves (the myelin coating) on the spine or in the brain (or both) in specific areas. In this case it appears to be nerves near the base of the spine.
It’s weird not feeling the syringe with the Copaxone going in to the belly. Whilst not feeling the injection sounds quite nice, it’s not exactly, is it? Not feeling your torso is disorientating at the moment and has other issues relating to it. I am hopeful, as in the previous attacks, that most of the feeling will come back over the next few weeks; but the return of the RRMS has left me pretty stressed to be honest.
One thing that came up in discussion was the issue I have with fatigue when standing up for over an hour or so (eg at a gig). It created much hilarity when the nurse suggested that one of the best ways to reduce the fatigue was to piss myself. I was quite taken aback by this suggestion until after some requests for repetition I found it was an accent issue and she’d actually meant ‘pace’. Much better idea I reckon.
They’ve written a letter for me which I hope to use to apply for an Access Card to help my when attending events (with better access to toilets and seats etc). I’d had to put off going to the Lottery Winners gig at Manchester Academy between Xmas and New Year because I was too worried that I wouldn’t find a place to sit (I was using a walking stick at the time). I was gutted at missing it but it was the correct decision at the time. We shall see whether I, a) get one and b) if it’s worth getting.
Another discussion was around possibly changing my medication from the three times a week Copaxone (glatiramer acetate) injections to daily tablets (Aubagio—terifluomide). When I first went for the injections it was partly due to the worry about purposely lowering your white blood cell count and also requiring regularly blood testing (not required with the Copaxone treatment). Given I am currently attacking myself again lowering the White Blood Cells doesn’t seem as bad an idea at all. The nurse is to call me back over the next few weeks and I am currently minded to opt for the change to Aubagio after the next batch of Copaxone is completed. We shall see.
Watch this space. In the meantime though I need to take some deep, deep breaths and try to stress less in general.
Physio 2
19/11/24 00:29
Went to physio for just the second time last week. It was a different practitioner than previously, and my next appointment is in just a few weeks. I’ve been given some different exercises to do—and this time their app was working which actually showed the exercises; and could be printed off and emailed to me. Definitely going to do them more regularly now and see what a difference it will make to my legs. It seems I really need to work on straightening the legs fully and that will largely be assisted through stretching the hamstrings out. Just straightening the legs I can feel the hamstrings do their stuff. Handily a few of the exercises can be done without the requirement of any equipment other than steps or a chair—and don’t need the resistance band. So I’ve no excuse not to do them at any point in the day that I can.
I dare say it is important to do it methodically rather than ad hoc though lest they won't get done properly. We’ll see how it goes this month anyway. Onwards and Upwards (with straight legs).
I dare say it is important to do it methodically rather than ad hoc though lest they won't get done properly. We’ll see how it goes this month anyway. Onwards and Upwards (with straight legs).
Card Carrying
18/11/24 12:11
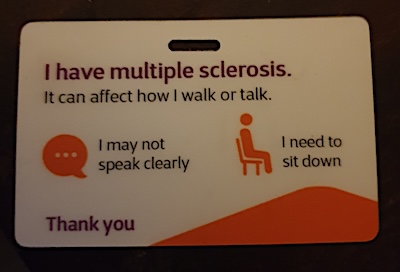
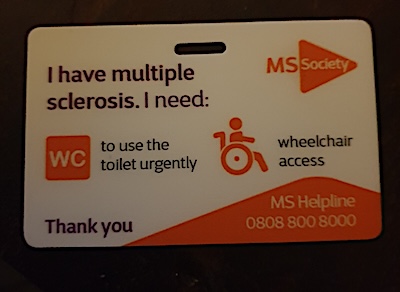
Last weekend I requested a card from the MS Society which I can use to show people if required that I suffer from MS. That followed the legs fatigue issue the other week. Thought it may come in handy when I am events and need to sit down—or an emergency toilet visit. It came in good time along with a booklet on fatigue. You can print one out from the website but I thought a plastic card would be much better in the long term.
The other reason for getting it is for using the train—especially at this time of the year when they have lots of staff stopping pissed people getting on train platforms. Having an explanation for wobbly legs which isn’t alcohol related could be most useful in December.
Hopefully I won’t need to pull out the card too often, but it’s nice to have one to hand.
Link to MS Society
The other reason for getting it is for using the train—especially at this time of the year when they have lots of staff stopping pissed people getting on train platforms. Having an explanation for wobbly legs which isn’t alcohol related could be most useful in December.
Hopefully I won’t need to pull out the card too often, but it’s nice to have one to hand.
Link to MS Society